Evidence based date wise workflow logs collated by the intern with clickable and verifiable links. Anecdotal self reflections on their internship learning with some video evidence of procedures performed
Evidence based date wise workflow logs collated by the intern with clickable and verifiable links.
Case 1:-
A 32 yr old male came with the complaints of fever since 1 week
HOPI
Patient was apparently asymptomatic 1 week back and then developed fever which was sudden in onset gradually progressive high grade associated with chills and generalised weakness for which he went to local RMP and took medication for 2 days still the symptoms didnot subside and further investigation like blood test done and his blood sugars were 300mg/dl
As the symptoms didnot subside they went to Miryalguda hospital there USG was done and impression showed HEPATIC ABSCESS
and refered to our hospital
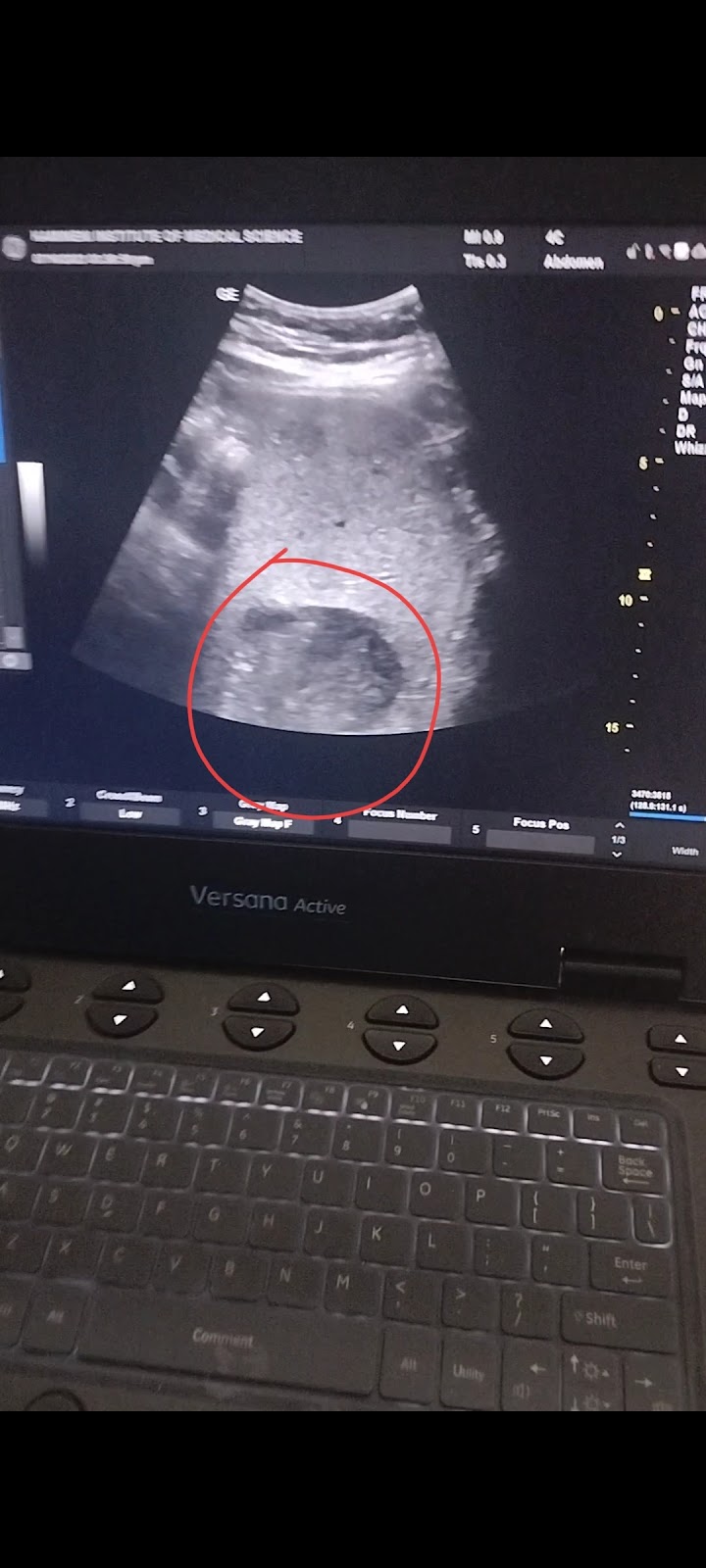
Patient came to hospital yesterday and USG was done impression showing:
NO H/o vomitings
No h/o cough cold diarrhoea
[10/7, 3:08 PM] Rakesh Biswas Sir HOD: Share the ultrasound video or image of his liver abscess asap
[10/7, 3:09 PM] Rakesh Biswas Sir HOD: Do the ultrasound yourself now.
[10/7, 3:09 PM] Gautham: Ok sir
[10/7, 3:47 PM] Rakesh Biswas Sir HOD: Try doing this from the back if this was done from the back
[10/7, 3:49 PM] Gautham: It was on the 5 6 segments of liver sir
[10/7, 3:50 PM] Rakesh Biswas Sir HOD: We are asking you about your probe placement in the patient's body
[10/7, 3:52 PM] Gautham: The probe was placed on Right hypochondrium region sir
[10/7, 3:54 PM] Rakesh Biswas Sir HOD: Now put it in the back right chest and share
[10/7, 3:54 PM] Gautham: Ok sir
[10/7, 8:04 PM] Rakesh Biswas Sir HOD: For a brief moment in the very beginning of the video here I'm not sure if you noticed how close the abscess was to your probe. So the learning point here is if you want to aspirate it after adequate liquefaction, you will need to approach it from this intercostal space
[10/7, 8:06 PM] Gautham: Yes sir
USG ON 6/10/23

FOLLOW UP :-
ON 21/10/23

On 3/11/23

1) List all the complaints of the patient with respect to the history and relevant clinical data ?
Ans: c/o fever since 1 week sudden in onset gradually progressive high grade associated with chills and generalised weakness
his blood sugars were 300mg/dl
Pain in the abdomen region.
Tenderness of right lumbar region .
Based on history how can we come to diagnosis of hepatic abscess?
right upper quadrant pain, fever
One of the DD is Hepatic abscess
2) Personal history of the patient??
Diet mixed
Appetite normal
Sleep Adequate
Bowel decreased since 3 days and passed stools yesterday
Bladder movements are regular
Addictions: occasional alcohol consumption since 5 years but stopped consumption from 2 months
Occasionally smoker since 5 years
3) Investigations done ?
USG -
Impression Hepatic abscess 9.3 x 7.9 cms with hyperechogenic lesion noted in 5th and 6th segments of liver with 20% liquifaction
CBP -
Hb 11.9gm/dl
TLC 13,900
Lymphocytes 55
Platelets 4.23
LFT -
TB 1.69
DB 0.40
SGOT 20
SGPT 47
ALP 314
Albumin 3.4
HbsAg Negative
4) Treatment given ?
TREATMENT:
Inj.NEOMOL 1G IV STAT
Inj.MAGNEX FORTE 1.5GMS IV STAT
Inj.METROGYL 500MG IV TID
Inj.PAN 40MG IV/OD
5) Why aspiration not done in our patient?
Indications of aspiration:
-Abscess should be > 10cms
-LIQUIFACTION should be more than 70%, but at present he has 40-50 % of liquifaction.
-Rapidly enlarging abscess
-Patient who are not responding to medications
Case 2 :-
[10/9, 9:23 AM] Gautham: 9/10/2023
Ward : AMC
Unit : 5
DOA : 7/10/2023
S :
Patient complaints of SOB on removing the oxygen mask.
fever spikes absent.
Pain in the abdomen region.
Tenderness of lateral and posterior aspect of abdomen subsided.
O:
Patient is conscious coherent and cooperative
-Pallor present.
-icterus present.
-clubbing, cyanosis, lymphadenopathy absent.
-oedema present pitting type on both lower limbs(below knee)
Vitals :
BP- 150/80mmHg
PR -88 bpm
RR-19 cpm
Temperature -98.6 F
SPO2 99 at 12 lt O2
CNS: NFND
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft, non tender.
A:
CKD on MHD
fluid overload with pulmonary edema
P:
1.fluid restriction less than 1lt/day
2.salt restriction less than 1.2gm/day
4.inj. HAI 5 units TID aa per advice
5. Tab. Nicardia 1mg po Tid
6.inj LASIX 40mg iv/BD
7. Tab NODOSIS 500 mg po/BD
8. Tab SHELCAL CT po/OD
9.Tab⋅ OROFER-XT. Po OD
10. INJ Iron Sucrose 200mg in 100ml NS Thrice weekly.
11.Inj. EPO 4K S/C twice weekly.
[10/9, 9:39 AM] Rakesh Biswas Sir HOD: Why did this diabetic land up in Ckd and dialysis within 7 years while there are many diabetics in our campus with 20 years and no complications or organ involvement? Can you try to look for the factors that make this patient different from them?
[10/9, 10:00 AM] Gautham: Sir the patient has both HTN and DM sir
[10/9, 10:01 AM] Gautham: The leading cause of CKD is mostly htn and DM sir
[10/9, 10:02 AM] Gautham: Due to these the inflammatory mediators act on blood vessels and nephrons
[10/9, 10:06 AM] Gautham: He also has muscle wasting and visceral fat which may aggregate the condition sir
[10/9, 10:32 AM] Rakesh Biswas Sir HOD: Which and why and how?
[10/9, 10:34 AM] Rakesh Biswas Sir HOD: How?
What is the scientific evidence for Sarcopenia and visceral fat combo leading to accelerated organ failure in diabetes?
Did the people doing well with their diabetes since 20 years have less visceral fat or Sarcopenia?
[10/9, 10:48 AM] Gautham: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8977978/
[10/10, 12:44 PM] Gautham: 10/10/2023
Ward : AMC
Unit : 5
DOA : 7/10/2023
S :
fever spikes absent.
Pain in the abdomen region.
Tenderness of lateral and posterior aspect of abdomen subsided.
O:
Patient is conscious coherent and cooperative
-Pallor present.
-icterus, clubbing, cyanosis, lymphadenopathy absent.
-oedema present pitting type on both lower limbs(below knee)
Vitals :
BP- 120/80mmHg
PR -82 bpm
RR-19 cpm
Temperature -98.6 F
SPO2 99 at 12 lt O2
CNS: NFND
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft, non tender.
A:
CKD stage v initiated on MHD with anaemia of chronic disease.
K/C/O type ll DM since 7 years and HTN since 1 year.
P:
1.fluid restriction less than 1lt/day
2.salt restriction less than 1.2gm/day
3 Tab. Nicardia 1mg po Tid
4.inj LASIX 40mg iv/BD
5. Tab NODOSIS 500 mg po/BD
6. Tab SHELCAL CT po/OD
7Tab⋅ OROFER-XT. Po OD
8. INJ Iron Sucrose 200mg in 100ml NS Thrice weekly.
9.Inj. EPO 4K S/C twice weekly.
[10/10, 12:47 PM] Gautham: https://www.mdpi.com/2673-8236/2/3/38
[10/11, 9:28 AM] Gautham: S :
fever spikes absent.
Pain in the abdomen region subsided.
Tenderness of lateral and posterior aspect of abdomen subsided.
O:
Patient is conscious coherent and cooperative
-Pallor present.
-icterus, clubbing, cyanosis, lymphadenopathy absent.
-oedema present pitting type on both lower limbs(below knee)
Vitals :
BP- 150/80mmHg
PR -82 bpm
RR-19 cpm
Temperature -98.6 F
SPO2 98 at 3 lt O2
CNS: NFND
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft, non tender.
A:
CKD stage v secondary to ? Diabetic nephropathy with anaemia of chronic disease With Heart failure reduced ejection fraction.
K/C/O type ll DM since 7 years and HTN since 1 year.
P:
1.fluid restriction less than 1.5 lt/day
2.salt restriction less than 2 gm/day
3 Tab. Nicardia 10mg po Tid
4.inj LASIX 40mg iv/BD
5. Tab NODOSIS 500 mg po/BD
6. Tab SHELCAL CT po/OD
7Tab⋅ OROFER-XT. Po OD
8. INJ Iron Sucrose 200mg in 100ml NS iv od
9.Inj. EPO 4K S/C once weekly.
10. Tab. Carvedilol 3.125 po od
11. Tab. ECOSPRIN AV 75/20 PO/HS
Anecdotal self reflections on their internship learning with some video evidence of procedures performed
This is about my learning skills in general medicine.
Although general medicine is all about vast knowledge, there are some cases where we have to apply our skill, which we will gain by experience.
Yeah I agree that the knowledge and skill are equally needed.
So if we experience more about the procedures then our self confidence will increase.
Sir I have done USG on a A 32 yr old male came with the complaints of fever since 1 week, who was diagnosed as HEPATIC ABSCESS.
And the following USG shows hepatic abscess on 5 and 6 segment with liquifaction of 20 % on 6/10/23.
And I have assisted in central line procedure (modified Seldinger technique).

And I have taken ABG samples

And also I have done other procedures like :-
1)Foley’s catheterisation
2)Ryles tube insertion
3)Assisting in Pleural tap
4)Assisted in Intubation
This is what I like about general medicine that learning has no endpoint, that we are students forever.


Comments
Post a Comment