A 53 year old came to casuality with C/o pedal edema since 2 months. C/O SOB Since 1 day. C/O decreased urine output since 2 months.
A 53 year old male came to casualty with chief
C/o pedal edema since 2 months
C/O SOB Since 1 day
C/O decreased urine output since 2 months.
History of presenting illness:-
Patient was apparently alright 1 year back then he developed decreased urine output for which he went to hospital and was diagnosed as chronic kidney disease and was on Conservative management.
Patient developed decreased urine output since 2 months.
No Hesitancy, dribbling of urine.
-History of pedal edema Since 2 months, pitting type upto knee.
-History of SOB since 1 day; Grade -IV according to MMRC , Orthopnea present, no PND.
No chest pain, no palpitations.
3. HISTORY OF PAST ILLNESS
K/c/o Dm-ll Since 7 years on insulin
K/c/o HTN Snce 1 year on CILNIDIPINE 10mg.
No history of asthma ,tuberculosis ,epilepsy
Personal history:
Diet mixed
Appetite normal
Sleep Adequate
Bowel are regular
Bladder movements decreased output since 2 months.
Addictions:
Alcohol - regular but stopped since 2 years
Smoking- 1 pack per day since 6 years.
General examination
Pat is c/c/c well oriented to time place person
He is moderately built and nourished
Mild pallor
Icterus present
No signs of cyanosis, clubbing, lymphadenopathy.
Edema (pitting type) is seen over B/L lower limbs below knee, lateral and posterior aspect of abdomen.
Vitals
Temperature - 98.4 F
BP - 130/90 mm hg
PR - 101 BPM
RR - 28 cpm
GRBS- 168 mg/dl
CVS - S1 S2 Heard no murmurs
RS - BAE + NVBS
CNS : NFND
P/A : soft,
Tenderness present over the swelling, which is developed over the lateral and posterior aspect of abdomen.






Provisional diagnosis:
CKD stage v initiated on MHD with anaemia of chronic disease.
K/C/O type ll DM since 7 years and HTN since 1 year.
Investigations:
6/10/23

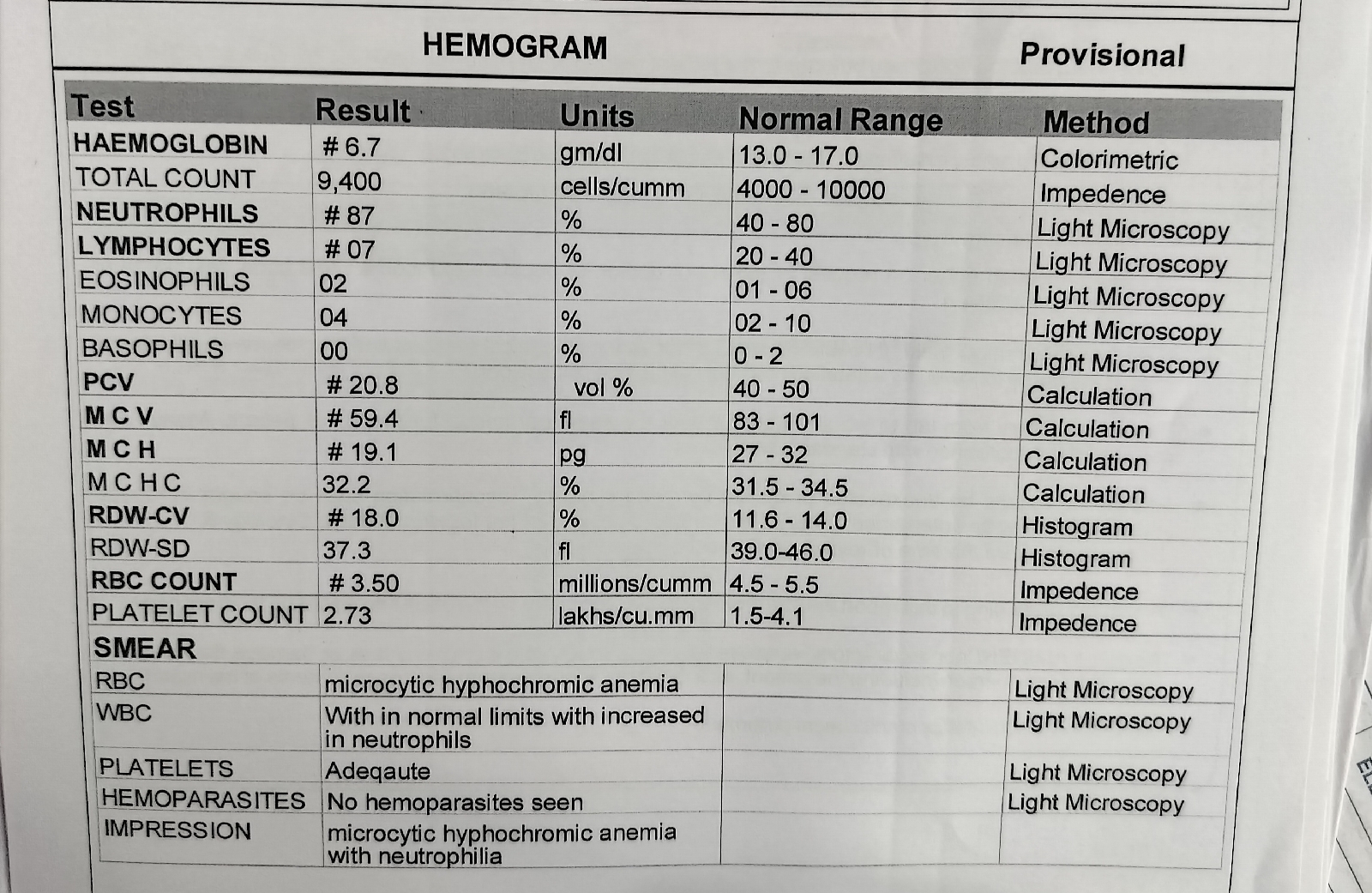











6/10/23
O/E :
Patient is c/c/c
BP-130/90
PR-101bpm
GRBS-168mg/dl
RR-28 cpm
CVS - S1S2 +
No murmurs
RS - BAE +, NVBS.
CNS- NFD
P/A- soft, Tenderness at the flanks
Treatment:
1. Inj. PAN 40 mg IV/OD
2. Tab. NODOSIS PO BD
3. Tab. shelcal - CT PO OD
4 TAb. OROFER-XT PO.OD
5. TAD. DOLD 650 MG PO SOS
6. GRBS monitoring
7. Monitor vitals 4th hourly
7/10/23
O/E :
Patient is c/c/c
BP-150/90
PR-98bpm
RR-18 cpm
CVS - S1S2 +
No murmurs
RS - BAE +, NVBS.
CNS- NFD
P/A- soft, Tenderness at the flanks.
Treatment:
1.fluid restriction less than 1lt/day
2.salt restriction less than 1.2gm/day
3.TAB CINOD 10mg PO BD
4.inj. HAI 5 units TID aa per advice
5. 7 (.) Grbs
6.inj LASIX 40mg iv/BD
7. Tab NODOSIS 500 mg po/BD
8. Tab SHELCAL CT po/OD
9.Tab⋅ OROFER-XT. Po OD
10. INJ Iron Sucrose 200mg in 100ml NS
Thrice weekly.
11.Inj. EPO 4K S/C twice weekly.
9/10/2023
Ward : AMC
Unit : 5
DOA : 7/10/2023
S :
Patient complaints of SOB on removing the oxygen mask.
fever spikes absent.
Pain in the abdomen region.
Tenderness of lateral and posterior aspect of abdomen subsided.
O:
Patient is conscious coherent and cooperative
-Pallor present.
-icterus present.
-clubbing, cyanosis, lymphadenopathy absent.
-oedema present pitting type on both lower limbs(below knee)
Vitals :
BP- 150/80mmHg
PR -88 bpm
RR-19 cpm
Temperature -98.6 F
SPO2 99 at 12 lt O2
CNS: NFND
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft, non tender.
9/10/2023
Ward : AMC
Unit : 5
DOA : 7/10/2023
S :
Patient complaints of SOB on removing the oxygen mask.
fever spikes absent.
Pain in the abdomen region.
Tenderness of lateral and posterior aspect of abdomen subsided.
O:
Patient is conscious coherent and cooperative
-Pallor present.
-icterus present.
-clubbing, cyanosis, lymphadenopathy absent.
-oedema present pitting type on both lower limbs(below knee)
Vitals :
BP- 150/80mmHg
PR -88 bpm
RR-19 cpm
Temperature -98.6 F
SPO2 99 at 12 lt O2
CNS: NFND
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft, non tender.
A:
CKD stage v initiated on MHD with anaemia of chronic disease.
K/C/O type ll DM since 7 years and HTN since 1 year.
P:
1.fluid restriction less than 1lt/day
2.salt restriction less than 1.2gm/day
4.inj. HAI 5 units TID aa per advice
5. Tab. Nicardia 1mg po Tid
6.inj LASIX 40mg iv/BD
7. Tab NODOSIS 500 mg po/BD
8. Tab SHELCAL CT po/OD
9.Tab⋅ OROFER-XT. Po OD
10. INJ Iron Sucrose 200mg in 100ml NS Thrice weekly.
11.Inj. EPO 4K S/C twice weekly
11/10/23
S :
fever spikes absent.
Pain in the abdomen region subsided.
Tenderness of lateral and posterior aspect of abdomen subsided.
O:
Patient is conscious coherent and cooperative
-Pallor present.
-icterus, clubbing, cyanosis, lymphadenopathy absent.
-oedema present pitting type on both lower limbs(below knee)
Vitals :
BP- 150/80mmHg
PR -82 bpm
RR-19 cpm
Temperature -98.6 F
SPO2 98 at 3 lt O2
CNS: NFND
CVS: S1,S2 heard , no murmurs.
RS: BAE, NVBS, no added sounds.
P/A: soft, non tender.
A:
CKD stage v secondary to ? Diabetic nephropathy with anaemia of chronic disease With Heart failure reduced ejection fraction.
K/C/O type ll DM since 7 years and HTN since 1 year.
P:
1.fluid restriction less than 1.5 lt/day
2.salt restriction less than 2 gm/day
3 Tab. Nicardia 10mg po Tid
4.inj LASIX 40mg iv/BD
5. Tab NODOSIS 500 mg po/BD
6. Tab SHELCAL CT po/OD
7Tab⋅ OROFER-XT. Po OD
8. INJ Iron Sucrose 200mg in 100ml NS iv od
9.Inj. EPO 4K S/C once weekly.
10. Tab. Carvedilol 3.125 po od
11. Tab. ECOSPRIN AV 75/20 PO/HS


Comments
Post a Comment