1801006109 Short case
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Cheif complaints:
A 14 year old female,resident of nagarjuna sagar presented with cheif complaints of
Pain in lower limbs (more in right knee) and lower back pain since 6 days
History of presenting illness:-
She was apparently asymptomatic 6days back then she developed pain in left ankle initially which is progressive and since 1 day she developed pain in both knee (more on the right side>>left) which is of throbbing type in nature .
Tenderness in calf muscles is present.
No aggravating and relieving factors
No history of fever ,abdominal pain
No H/o of swelling, weakness.
All the peripheral pulses are palpable
No h/o chest pain,shortness of breath,headache and palpitations
No h/o aphasia or dysphagia, seizures,Severe headache,altered mental status
BIRTH HISTORY:
Second child
Consanguineous 3 rd degree
All trimesters were uneventful.
-She was delivered through Caeserean section
-Birth weight of 3kg.
PAST HISTORY -
At the age of 3 she had complaints of fever,sob,fatigue, patient was diagnosed as sickle cell anemia since then She underwent multiple PRBC transfusion 20times in 11years last PRBC transfusion was in jan 2023.
H/O similar Complaints in the past for 3 times.
H/O jaundice 2yrs ago
H/O cholelithiasis 3months ago
Not a Known case of DM,HTN,CAD,CVA, EPILEPSY
IMMUNIZATION HISTORY
BCG scar present.
patient is immunised till date
PERSONAL HISTORY :
Diet: mixed
Appetite: normal
Sleep: adequate
Bowel and bladder movements regular
No addictions
FAMILY HISTORY -
3rd degree consanguity of parents
No known affected relatives
GENERAL EXAMINATION:
Patient was conscious, coherent and cooperative.
Well oriented to time, place and person.
Moderately built and nourished.
Pallor present
Icterus present
Cyanosis, clubbing, lymphadenopathy, Pedal edema absent
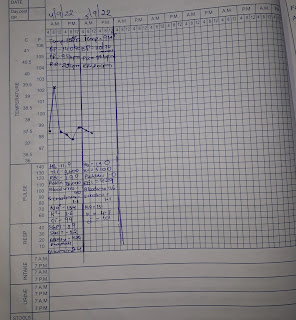
Vitals
Temp: Afebrile
PR- 96bpm
RR- 18/Min
BP- 110/70 mmHg
SYSTEMIC EXAMINATION
P/A - Shape of abdomen- Normal. Umbilicus everted. No scars. No organomegaly. Bowel sounds heard.
CVS examination -
-Inspection
Shape of chest- elliptical shaped chest
No engorged veins, scars, visible pulsations
No JVP
•Palpation
Apex beat can be palpable in 5th inter costal space medial to mid clavicular line
•Auscultation
S1,S2 are heard
no murmurs
RS- NVBS.
CNS- No focal neurological deficits
Tone, power and reflexes are normal.
On examination on lower limbs bilateral calf tenderness is seen.
Clinical pictures:





Peripheral smear

X ray



Provisional diagnosis:-
Hemolytic Anaemia ?
INVESTIGATIONS :-
Hemoglobin-8gm/dl
TLC-22,900
PCV-23.1(normal-36 to 46)
BLOOD group -O positive
Total bilirubin-20.15
Direct bilirubin-14.13
SGOT-170
SGPT-180
ALP-560
CRP-negative
Serology -negative
LDH-
blood urea-20mg/dl
Creatinine-0.4
Electrtrolytes-
sodium- 136 mEq/l
Pottasium-4.5 mEq/l
Chloride-101mEq/l
Calcium 1.02mmol/l
Peripheral smear-
Anisopoikilocytosis with predominant Sickle cell, normocytes, few microcytes
Platelets and wbc were raised



Final diagnosis:-
Sickle cell anaemia with vaso occlusive crisis.
Treatment:-
IV FLUID IONS@75ml/hr
TAB.FOLIC ACID 5mg PO OD
TAB.ECOSPRIN 75mg PO OD
TAB.HYDROXY UREA 1000 PO OD
INJ.TRAMADOL 1Amp in 100ml NS SOS
INJ.PANTOP 40mg IV OD
INJ.ZOFER 4mg IV SOS
TAB.NAPROXEN 250mg PO BD


Comments
Post a Comment